
One of the patterns I have noticed repeatedly in clinical practice is that many people come to physiotherapy wanting to feel better. That makes complete sense. When pain is affecting your work, hobbies, sleep, or ability to care for your family, relief often feels like the most important goal.
Over time, however, I have come to realise that feeling better and getting better are not always the same thing.
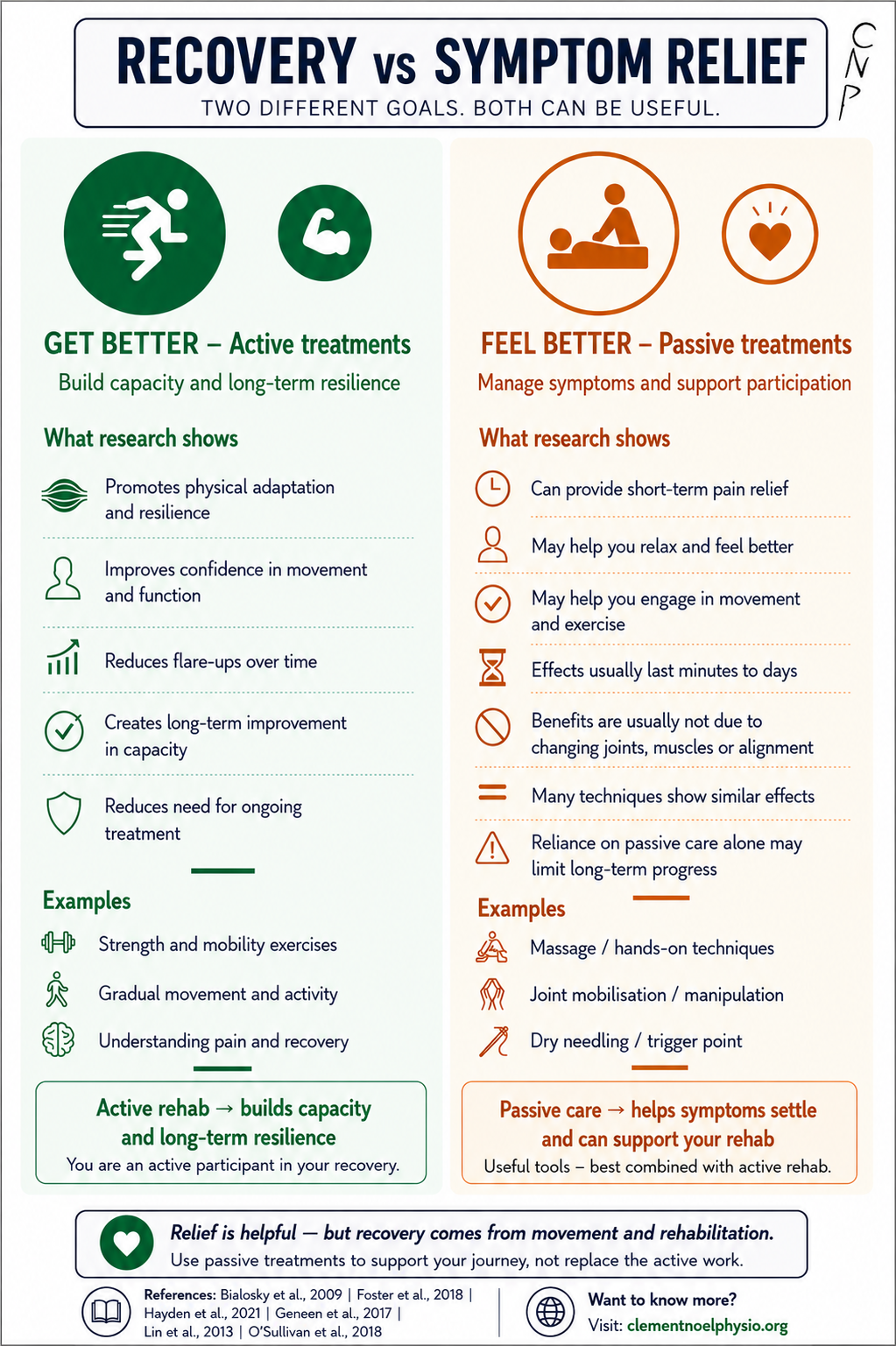
This infographic was created to help explain that distinction.

A common pattern goes something like this: someone arrives in pain and asks for massage, dry needling, manipulation, or another hands-on treatment because it has helped before. The treatment provides relief, sometimes for a few hours, sometimes for a few days. Then the pain returns. Another treatment follows, then another. Eventually frustration builds because despite temporarily feeling better, the person does not feel they are actually improving. In many cases, the issue is not that the treatment failed. The issue is that symptom relief was mistaken for recovery.
My own thinking on this topic has evolved over the years. Early in my career, I probably focused more on helping people feel better. As I learned more about rehabilitation, pain science, and behaviour change, I gradually shifted towards exercise, self-management, and building long-term capacity. At times, I may even have gone too far in that direction and underestimated the value of symptom relief and support. These days, I find myself somewhere in the middle. I still believe lasting recovery generally requires active participation, but I have also come to appreciate that people are not machines. Sometimes pain is overwhelming, life is stressful, and a little relief or reassurance can make all the difference.
The challenge is finding the balance.
This is why I do not see passive treatments as the enemy. Massage, manual therapy, dry needling, and similar approaches can reduce pain, improve comfort, and help people feel supported. They can also create an opportunity to move more comfortably and engage with rehabilitation. The problem arises when they become the entire treatment plan. Recovery usually requires adaptation, and adaptation rarely occurs because someone performs a treatment to us. It tends to occur when we gradually rebuild strength, fitness, confidence, movement options, and trust in our bodies through movement, activity, learning, and experience.
One of the goals I increasingly value as a clinician is helping people become less dependent on healthcare. This is not because support is bad, but because independence is often empowering. When people develop the confidence and skills to manage many challenges themselves, they spend less time attending appointments, less money seeking ongoing treatment, and often feel more in control of their health. There is also a broader perspective worth considering. Every appointment, journey to a clinic, and healthcare intervention carries a financial and environmental cost. Helping people become less reliant on ongoing treatment is therefore not only beneficial for them, but also contributes to a more sustainable healthcare system.
The research behind this infographic points in a similar direction. Studies exploring manual therapy suggest that many of its benefits are likely related to pain modulation, expectations, and other neurophysiological effects rather than structural corrections or “realignment” of the body (Bialosky et al., 2009). Contemporary low back pain research emphasises physical activity, self-management, and person-centred care over passive treatments alone (Foster et al., 2018; O’Sullivan et al., 2018). Reviews of exercise therapy consistently show that movement can improve pain, function, quality of life, and physical capacity in people with persistent musculoskeletal conditions (Geneen et al., 2017; Hayden et al., 2021). Meanwhile, research into public beliefs about back pain highlights the importance of education in challenging misconceptions around posture, imaging findings, structural damage, and fragility (Lin et al., 2013).
Ultimately, the message of the infographic is not that passive treatments are bad and exercise is good. The reality is more nuanced than that. Passive treatments can provide relief, comfort, reassurance, and support. Active rehabilitation helps build capacity, confidence, resilience, and independence. Both can have a place in care. The important question is whether the treatment is helping someone move towards greater participation in life and less reliance on healthcare over time.
The longer I work in physiotherapy, the less interested I become in choosing sides between active and passive care. Instead, I find myself asking a different question: is this helping the person in front of me move towards recovery?
Sometimes that means helping them feel better today. Sometimes it means helping them build the capacity they will need tomorrow.
Usually, it means a little bit of both.
References
Bialosky, J. E., Bishop, M. D., Price, D. D., Robinson, M. E., & George, S. Z. (2009). The mechanisms of manual therapy in the treatment of musculoskeletal pain: A comprehensive model. Manual Therapy, 14(5), 531–538. https://doi.org/10.1016/j.math.2008.09.001
Foster, N. E., Anema, J. R., Cherkin, D., Chou, R., Cohen, S. P., Gross, D. P., Ferreira, P. H., Fritz, J. M., Koes, B. W., Peul, W., Turner, J. A., Maher, C. G., & Lancet Low Back Pain Series Working Group (2018). Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet (London, England), 391(10137), 2368–2383. https://doi.org/10.1016/S0140-6736(18)30489-6
Geneen, L. J., Moore, R. A., Clarke, C., Martin, D., Colvin, L. A., & Smith, B. H. (2017). Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. The Cochrane database of systematic reviews, 4(4), CD011279. https://doi.org/10.1002/14651858.CD011279.pub3
Hayden, J. A., Ellis, J., Ogilvie, R., Malmivaara, A., & van Tulder, M. W. (2021). Exercise therapy for chronic low back pain. The Cochrane database of systematic reviews, 9(9), CD009790. https://doi.org/10.1002/14651858.CD009790.pub2
Lin, I. B., O’Sullivan, P. B., Coffin, J. A., Mak, D. B., Toussaint, S., & Straker, L. M. (2013). Disabling chronic low back pain as an iatrogenic disorder: a qualitative study in Aboriginal Australians. BMJ open, 3(4), e002654. https://doi.org/10.1136/bmjopen-2013-002654
O’Sullivan, P. B., Caneiro, J. P., O’Keeffe, M., Smith, A., Dankaerts, W., Fersum, K., & O’Sullivan, K. (2018). Cognitive Functional Therapy: An Integrated Behavioral Approach for the Targeted Management of Disabling Low Back Pain. Physical therapy, 98(5), 408–423. https://doi.org/10.1093/ptj/pzy022
{kind=link}
Also Available in other languages!
FRENCH 🇫🇷 :
{kind=link}
Discover more from A physiotherapist's learning journey
Subscribe to get the latest posts sent to your email.
Leave a Reply